Kidney Drug Safety Calculator
Check Your Medication Safety
Enter your current eGFR value and select medications you take to see if your doses need adjustment for kidney disease.
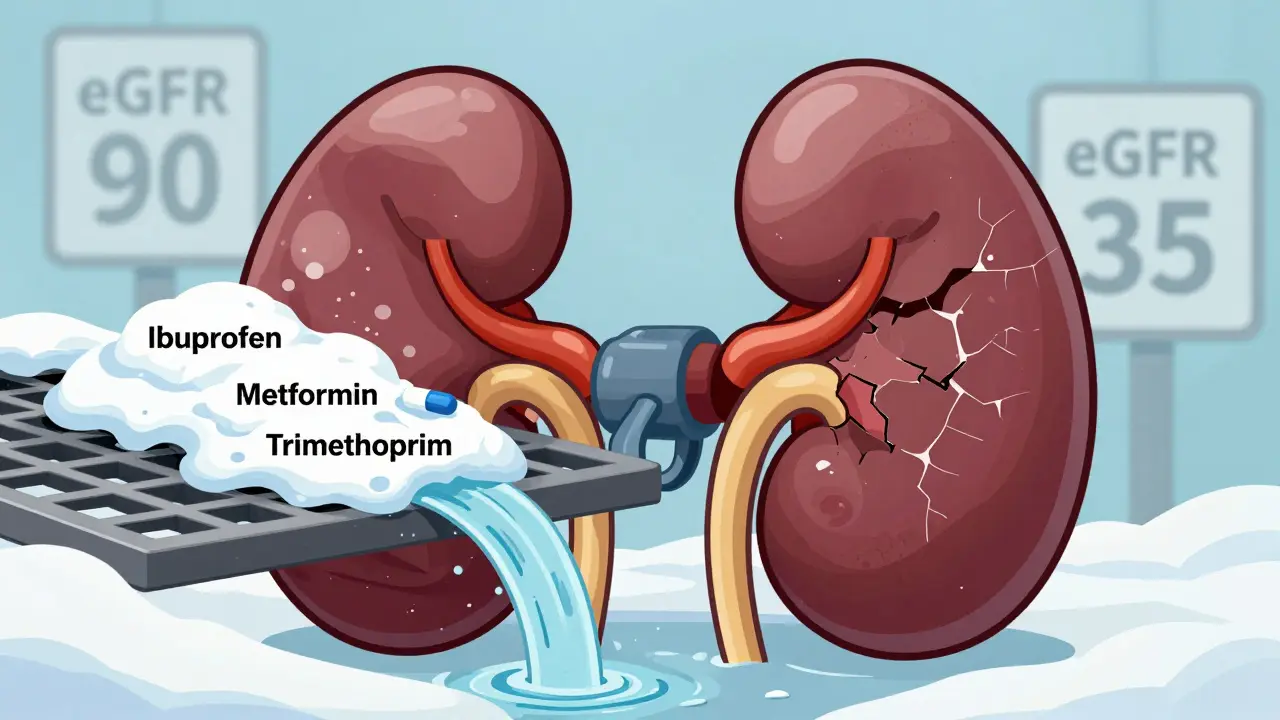
When your kidneys aren't working right, your meds can turn against you. It’s not just about taking pills - it’s about how much you take, and whether your body can clear it out. For someone with chronic kidney disease (CKD), even a standard dose of ibuprofen or metformin can pile up like unshed snow in a clogged gutter. And when that happens, the consequences aren’t just uncomfortable - they can be deadly.
Why Your Kidneys Are the Gatekeepers of Your Medications
Your kidneys don’t just make urine. They filter about 30% of all medications you take. That includes antibiotics, painkillers, diabetes drugs, blood thinners, and even some heart medications. When kidney function drops - say, from normal (eGFR >90) to stage 3 CKD (eGFR 30-59) - that filtration system starts to slow. Drugs that used to leave your body in 6 hours now hang around for 12, 24, even 48 hours. That’s not a glitch. It’s a buildup. And buildup leads to toxicity.Think of it like this: if your kidneys are 40% damaged, your body can’t flush out drugs the way it used to. So a dose that was safe last year becomes dangerous today. The National Kidney Foundation says 37 million Americans have CKD. Many don’t even know it. And that’s the real problem - doctors often prescribe based on old habits, not current kidney function.
Drugs That Turn Dangerous in CKD
Not all medications are created equal when your kidneys are failing. Some are fine. Others? They’re ticking time bombs.- NSAIDs (ibuprofen, naproxen, diclofenac): These are the #1 offender. Even a few days of regular use can spike creatinine levels and trigger acute kidney injury. In people with eGFR under 60, NSAIDs raise AKI risk by 3 times. In stage 4 or 5 CKD? Avoid them completely. One Reddit user, @KidneyWarrior2022, saw his creatinine jump from 1.8 to 3.2 after taking standard ibuprofen for back pain. He spent 5 days in the hospital.
- Metformin: This common diabetes drug is usually safe - until eGFR falls below 45. Below 30? Stop it. Why? Because it can cause lactic acidosis, a rare but deadly condition where your blood turns acidic. But here’s the twist: a Cochrane review of 20,000 patients found zero cases of lactic acidosis when dosing rules were followed. The risk isn’t the drug - it’s the lack of adjustment.
- Sulfonylureas (chlorpropamide, glyburide): These older diabetes pills are especially risky. Chlorpropamide’s half-life jumps from 34 hours to over 200 hours in stage 5 CKD. That means one dose can cause severe low blood sugar for days. Glyburide’s active metabolite sticks around so long it can trigger hypoglycemia for over 72 hours. Glipizide? Safer. It’s cleared through the liver, not the kidneys.
- Trimethoprim (and co-trimoxazole): This antibiotic is often used for UTIs. But if you’re also on an ACE inhibitor or ARB (common for high blood pressure and kidney protection), trimethoprim can push your potassium into the danger zone. Studies show potassium levels rise 1.2-1.8 mmol/L within 48 hours. That’s enough to cause heart rhythm problems - or worse.
- Aciclovir: Used for shingles and herpes, this drug can form crystals in your kidney tubules. In people with eGFR under 50, up to 15% develop crystal nephropathy. Symptoms? Confusion, seizures, kidney failure. All from a standard dose that’s fine for healthy kidneys.
- DOACs (apixaban, rivaroxaban): These newer blood thinners are popular because they don’t need frequent blood tests. But 50% of apixaban and 33% of rivaroxaban are cleared by the kidneys. In stage 4 CKD, bleeding risk spikes 40% compared to stage 2. Warfarin? It’s metabolized by the liver, so it’s often safer in advanced CKD - if monitored properly.
- Tacrolimus and cyclosporine: Lifesavers for transplant patients. But their therapeutic window is razor-thin. Just 20-30% above the safe level causes toxicity. Chronic use leads to permanent scarring of the kidneys in 25-30% of transplant recipients. Dosing here isn’t just science - it’s art.
How Doctors Miss the Mark
You’d think doctors would check kidney function before prescribing. But they don’t always. A JAMA Internal Medicine study found that in 35% of primary care visits, doctors relied only on serum creatinine - not eGFR. That’s like judging a car’s fuel efficiency by looking at the gas gauge, not the odometer. Serum creatinine can look normal even when kidney function is half gone.Another big issue? Polypharmacy. CKD patients take an average of 10-12 medications daily. That’s not because they’re overmedicated - it’s because they’re managing diabetes, heart disease, high blood pressure, anemia, and bone disease. Each drug has its own clearance pathway. Some are nephrotoxic. Others interact. The result? A perfect storm.
And then there’s the “out of sight, out of mind” problem. If a patient hasn’t been in the hospital in two years, providers assume their kidney function is stable. But CKD is progressive. A dose that was safe last year might be lethal now.
The Numbers Don’t Lie
Drug-induced kidney injury isn’t rare. It’s common. And it’s preventable.- 14-26% of all acute kidney injuries in hospitals are caused by medications.
- 19-29% of all AKI cases in hospitalized patients are linked to drugs - and those patients are 1.8 times more likely to die than those with AKI from other causes.
- 78% of CKD patients surveyed by the American Association of Kidney Patients received at least one medication without proper dose adjustment.
- 43% of those patients had adverse events serious enough to require emergency care.
- Drug-induced AKI adds $10,000-$15,000 per hospital stay. Preventable cases cost the U.S. system $18.7 billion a year.
These aren’t abstract numbers. These are people - your neighbor, your parent, your friend - who were given the wrong dose of a common pill. And they paid the price.
What You Can Do
If you or someone you care for has CKD, here’s what matters:- Know your eGFR. Not creatinine. Not “kidney numbers.” Your eGFR. Ask for it at every appointment. If they say “your kidneys are fine,” ask: “What’s my eGFR?” If it’s below 60, all your meds need a second look.
- Ask: “Is this drug cleared by the kidneys?” If yes, ask: “Do I need a lower dose?” Many drugs have clear guidelines. If your doctor doesn’t know, ask for a pharmacist.
- Map your meds. Write down every pill, supplement, and OTC drug. Include frequency and dose. Bring it to every appointment. Highlight NSAIDs, antibiotics, and diabetes drugs.
- Use tools. Apps like Meds & CKD (from Healthmap Solutions) flag risky combinations and show safe dosing based on your eGFR. Users report 82% better communication with providers.
- Speak up. If you feel dizzy, confused, nauseated, or have irregular heartbeat after starting a new drug - call your doctor. Don’t wait. These can be signs of drug buildup.

What’s Changing - and What’s Coming
The system is starting to catch up. The FDA now requires all new drugs to include renal dosing info on their labels. In 2021, Pfizer was fined $2.5 million for failing to label kidney risks properly. That’s a signal: this isn’t optional anymore.Technology is stepping in too. KidneyIntelX, approved by the FDA in 2023, uses machine learning to predict your personal risk of drug toxicity based on your eGFR, age, weight, and other meds. It’s 89% accurate. And it’s just the start.
Stanford’s Dr. Richard Lafayette predicts that within five years, electronic health records will automatically block unsafe prescriptions for CKD patients. Imagine: you walk in for a refill, and the system says, “This dose is unsafe. Adjust to 5 mg daily.” That’s not science fiction. It’s coming.
Meanwhile, the KDIGO 2024 guidelines (coming this fall) will expand recommendations for newer drugs like SGLT2 inhibitors - which actually protect the kidneys, but still need dose tweaks when eGFR drops below 45.
Final Thought
Kidney disease doesn’t have to be a death sentence. But medication mismanagement? That’s preventable. The problem isn’t the drugs. It’s the lack of attention to how your body changes. Your kidneys don’t work the same as they did five years ago. Your meds shouldn’t either. Simple steps - knowing your eGFR, asking the right questions, using tools - can keep you out of the hospital. And that’s worth more than any pill.Can I still take ibuprofen if I have kidney disease?
If your eGFR is below 60 mL/min/1.73m² (stage 3 CKD or worse), avoid ibuprofen and other NSAIDs entirely. They reduce blood flow to the kidneys and can cause sudden kidney injury. Even short-term use can lead to hospitalization. Safer alternatives include acetaminophen (Tylenol), but always check with your doctor first.
How do I know if my medication dose needs to be adjusted?
If your eGFR is below 60, at least 40% of commonly prescribed drugs need a dose change. Look for drugs labeled as "primarily renally cleared" or check databases like the University of California San Francisco’s Renal PharmPK. Ask your pharmacist or nephrologist to review all your medications. Never assume a standard dose is safe.
Is metformin safe for people with kidney disease?
Metformin is safe if dosed correctly. Reduce the dose when eGFR drops below 45, and stop it completely if eGFR falls below 30. The risk of lactic acidosis is extremely low - only when guidelines are ignored. A Cochrane review of 20,000 patients found no cases of lactic acidosis when dosing rules were followed. Always monitor kidney function regularly.
Why do some diabetes drugs cause low blood sugar in kidney disease?
Drugs like chlorpropamide and glyburide are broken down and cleared by the kidneys. When kidneys fail, these drugs and their active metabolites build up in the blood. That overstimulates insulin release, causing prolonged, severe low blood sugar - sometimes lasting over 72 hours. Glipizide and linagliptin are safer because they’re cleared by the liver, not the kidneys.
Can over-the-counter supplements harm my kidneys?
Yes. Many herbal supplements, including St. John’s Wort, licorice root, and certain weight-loss teas, contain compounds that are toxic to kidneys or interfere with medications. Some raise potassium, others cause direct damage. Always tell your doctor what supplements you take - even if they say "natural."
What’s the best way to track my medication risks?
Use a dedicated app like Meds & CKD, which lets you enter your eGFR and lists which of your meds are risky. You can also ask your pharmacist for a medication review. Keep a printed list of all your drugs, including doses and reasons, and bring it to every appointment. Many patients report better communication and fewer side effects after doing this.



March 2, 2026 AT 08:56 AM
So let me get this straight. I can't take ibuprofen for my back pain but my doctor keeps prescribing it like it's candy. Thanks for the reminder that my kidneys are basically a broken filter and I'm just one Advil away from a hospital stay. Classic.
And why do I need an app to tell me what my own body is doing? Because the system is broken. Not my kidneys. The system.
March 3, 2026 AT 22:56 PM
This is a meticulously researched and sobering exposition on a critical public health oversight. The data presented underscores a systemic failure in clinical practice, wherein renal function is routinely under-assessed despite its profound implications for pharmacokinetics. The correlation between medication mismanagement and preventable acute kidney injury is both statistically significant and ethically indefensible. A call for mandatory eGFR verification prior to prescribing is not merely prudent-it is imperative.
March 4, 2026 AT 23:14 PM
I read this whole thing and honestly? I'm just glad I don't have kidney issues. But yeah, NSAIDs are bad. I knew that. My cousin went to the ER after taking ibuprofen for a week. He was like 'it's just painkillers' and now he's on dialysis. Dumb. Don't be dumb. Check your eGFR. Simple.
Also, metformin? Yeah, if you're not a diabetic, stop taking it. It's not a vitamin.
March 6, 2026 AT 16:34 PM
I’ve seen this play out in three different countries. In the U.S., it’s about forgetting to check labs. In the UK, it’s about time constraints. In Australia? It’s about patients not speaking up. The pattern is the same: nobody’s talking. Nobody’s listening. And someone ends up in the ICU because a pill was dosed like they were 30 and healthy.
It’s not the drug. It’s the silence.
March 7, 2026 AT 17:16 PM
I’m a nurse and I’ve watched this happen too many times. Elderly patients on 12 meds, no one reviews them, and then they get confused or fall. We blame dementia. But it’s often drug buildup. I hand out printed lists to every CKD patient I see. They’re so grateful. Just one sheet of paper can save a life. It’s not complicated. It’s just not prioritized.
March 9, 2026 AT 10:18 AM
So basically, if you’re over 50 and on any meds, you’re one prescription away from becoming a statistic. Cool. Thanks for the heads up. Now I’ll just stop taking all my pills and hope for the best.
March 9, 2026 AT 20:57 PM
I love how this post doesn’t just list the dangers-it gives you the tools. Knowing your eGFR isn’t optional. It’s your lifeline. I used to think my doctor knew what I was on. Turns out, he didn’t. I printed my med list, walked into his office, and said, 'Explain every one.' He paused. Then he apologized. That’s the power of being loud.
March 11, 2026 AT 00:44 AM
I have stage 3 CKD. I’ve been on metformin for 12 years. My last eGFR was 42. I didn’t know I needed to adjust. I didn’t even know to ask. This post saved me from a hospital trip. I called my pharmacist today. They adjusted my dose. It’s that simple. I wish I’d known this five years ago.
March 12, 2026 AT 17:25 PM
If your kidneys are slow, your meds stay longer. That’s it. No magic. No mystery. Just math. Check your eGFR. If it’s under 60, ask your doc: 'Is this safe?' If they say 'probably,' ask again. Better safe than dead.
March 12, 2026 AT 23:05 PM
I use Meds & CKD. It flagged my blood pressure med as risky. I showed it to my nephrologist. She changed it. No drama. No panic. Just a better plan. It’s not about fear. It’s about awareness.
March 13, 2026 AT 05:10 AM
This is the kind of info that should be on every prescription bottle. Not just for CKD patients-for everyone. I didn’t know my grandma was on a drug that could wreck her kidneys. She’s 78. She takes 8 pills a day. I’m gonna sit her down this weekend and go through them. She’s lucky she has me. Others aren’t.
March 13, 2026 AT 08:10 AM
I don’t trust any of this. The FDA, the doctors, the apps-they’re all part of the system. They want you dependent. They want you scared. They don’t care if you live or die. They just want your money. I stopped all my meds and started drinking lemon water. My eGFR went up. Coincidence? I think not.